Lupine Publishers| Journal of Neurology and Brain Disorders
Abstract
Background: The SARS-CoV-2 virus causes a wide
spectrum of disease severity. Initial manifestations include fever, dry cough,
and constitutional symptoms, which may progress to respiratory disease. There
may also be neurological and psychiatric manifestations, involving both the
central and peripheral nervous system.
Methods: We performed a literature search of
the databases PubMed, EMBASE, The Cochrane Library and Web of Science for
observational studies reporting neurological, psychiatric, and neuropsychiatric
effects of COVID-19. This was followed by a narrative synthesis to summarise
the data and discuss neuropsychiatric associations, symptom severity, management,
and recovery.
Findings: The most frequently reported
neurological symptoms were ageusia, hyposmia/anosmia, dizziness, headache, and
loss of consciousness. Statistically significant relationships were noted
between Asian ethnicity and peripheral neuropathy (p=0·0001) and
neuro-syndromic symptoms (p=0·001). ITU admission was found to have a
statistically significant relationship with male sex (p=0·024). Depression and
anxiety were also identified both during and after infection. The most frequent
treatments used were intravenous immunoglobulins, followed by antibiotics,
antivirals, and hydroxychloroquine; with mean treatment duration of 6 days.
Interpretation: Various
neuropsychiatric symptoms have been associated with COVID-19 infection. More
studies are required to further our knowledge in the management of neurological
and psychiatric symptoms during and after COVID-19 infection
Funding: This research received no specific
grant from any funding agency in the public, commercial, or not-for-profit sectors.
Introduction
Severe
acute respiratory syndrome coronavirus 2 (SARSCoV- 2) is a novel virus,
initially discovered in the city of Wuhan, China [1]. SARS-CoV-2 causes
coronavirus disease (COVID-19), which has led to an ongoing global pandemic.
Despite belonging to the coronavirus family, which usually cause self- limiting
upper respiratory tract infections, SARS-CoV-2 is often more virulent than most
coronaviruses and may lead to severe respiratory disease [2].
The
mechanism of action for SARS-CoV-2 may relate to a specific tropism for
respiratory tract mucosal cells through the attachment of viral surface
proteins to angiotensin-converting enzyme (ACE) 2 receptors [3]. After
infection, the virus causes a wide spectrum of disease severity, with most patients
suffering a mild self-limiting disease. Initial manifestations include fever,
dry cough and constitutional symptoms (headache, fatigue, myalgia, arthralgia),
progressing to respiratory disease of mild to moderate severity [2,4]. Other
disease manifestations include gastrointestinal symptoms (nausea, vomiting,
diarrhoea), sore throat, skin rashes, anosmia, ageusia, and chest pain [5]. In
patients with underlying comorbidities or advanced age, the infection may be
complicated with acute respiratory distress syndrome (ARDS), acute renal
failure, sepsis, multi-organ failure and death [6,7]. As the pandemic of
COVID-19 persists, the knowledge of the clinical disease spectrum is still
unfolding. Medical literature of COVID-19 infected patients reveals a variety
of extra-pulmonary organ involvement [8]. Among these, COVID-19 has been
associated with several neurological and psychiatric effects, involving both
the central and peripheral nervous system [9].
Methods
This
systematic review follows the Preferred Reporting Items for Systematic reviews
and MetaAnalyses (PRISMA) statement [10] and was registered in the PROSPERO
International Prospective Register of Systematic Reviews (number CRD42020203770
at www.crd.york.ac.uk/PROSPERO).
Search Strategy
The
literature search was performed in August 2020 using the databases PubMed,
EMBASE, The Cochrane Library and Web of Science, from their respective
inception dates. The following search terms were used:
(Neuro*
OR Nervous OR Psychiatry* OR Mental) AND (COVID OR Corona*)
The
search strategies incorporated both medical subject headings (MeSH) and
free-text terms, which were adapted according to the database searched. Grey
literature was also searched. Reference lists of the identified papers and
reviews were hand-searched. Publication languages included English and Greek.
There were no publication period restrictions.
Inclusion and Exclusion Criteria
Included
studies were observational studies reporting neurological, psychiatric, and
neuropsychiatric effects of COVID-19. The included participants were COVID-19
patients of any ethnic origin, sex/gender, age, country, and were either
actively infected from COVID-19 at the time of the study or had recovered. We
did not include studies examining psychiatric effects on the general population
as an indirect result of the pandemic.
Main Outcomes
The
main outcomes included neurological, psychiatric, and neuropsychiatric effects
of COVID-19, either based on clinical diagnosis or relevant diagnostic
questionnaires. Information about recovery and treatment was reported when
available.
Screening
Titles
were screened for inclusion, followed by screening of abstracts, and then
content. One author (SS) screened the papers, and any disagreements were
resolved by discussion with the review’s primary author (MS) and the other
authors.
Data Extraction
The
Cochrane good practice data extraction form was used for data extraction. Data
extraction from reviews involved the NICE extraction form, and the data were
extracted in an electronic format.
Risk of Bias/Quality Assessment
The
quality and risk of bias were assessed by the Mixed Methods tool for Appraisal
(MMAT). The guidance from the Centre for Reviews and Dissemination was used for
the appraisal of review papers. Discrepancies were resolved by discussion
within the authors’ team.
Strategy for Data Synthesis
We
performed a narrative synthesis review of original studies and reviews
reporting neurological, psychiatric, and neuropsychiatric effects in COVID-19
patients.
We
summarised the data and discussed:
a)
Neuropsychiatric associations
b)
Symptom severity
c)
Management and
d)
Recovery
Information
from the various identified studies was analysed, summarised, and compared.
Results
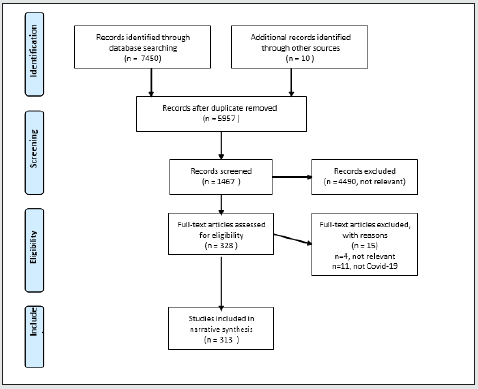
Following
our literature search, we identified a total of 7,460 papers. After removing
the duplicated and irrelevant papers, 328 full text articles remained to be
assessed for eligibility using the inclusion and exclusion criteria. Of these,
313 studies were included in the final narrative synthesis: specifically, 307
studies for neurological symptoms and 7 studies for psychiatric symptoms, as
shown in Figure 1. A total of 15 full text papers were excluded as they were
either not relevant (n=4) or unrelated to COVID-19 infection (n=11).
Figure 1: PRISMA flowchart of selected studies.

Neurological Symptoms
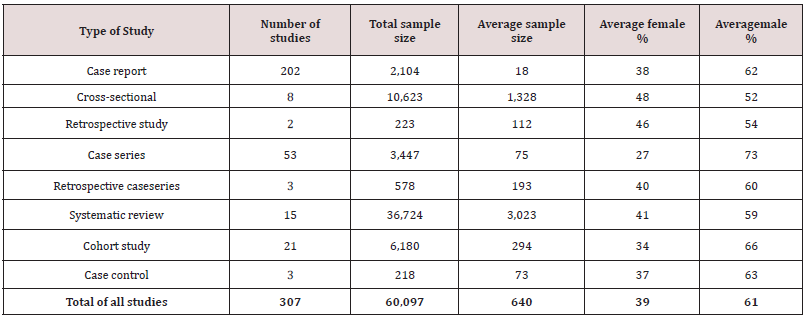
A
total of 307 studies for neurological symptoms were included in the narrative
synthesis, as mentioned above, of which 202 were case reports, 53 case series,
2 retrospective studies, 21 cohort studies, 15 systematic reviews, 8
cross-sectional studies, 3 casecontrol studies, and 3 retrospective case
series. A summary of the studies included in the systematic review is shown in
Table 1, and a complete list of the studies is provided in Supplementary
Material 1. The mean age of the patients included was 55·11 (±17.91) years.
Most of the patients in our cohort were males (61%) and the majority of the
participants were Asians (57%).
Table 1: Summary
of studies included in the systematic review for neurological symptoms.

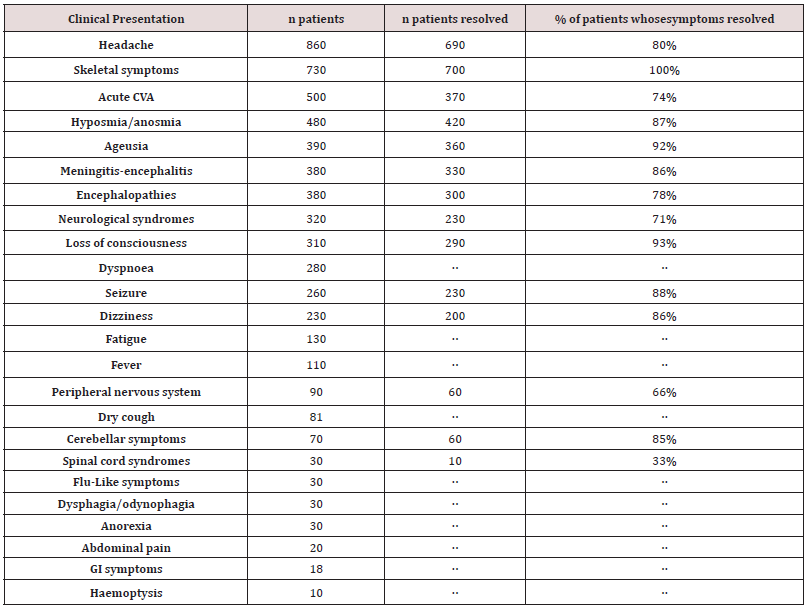
Clinical Presentation
A
total of 107 studies (42·7%), involving 26,758 patients, included a full
account of neurological symptoms experienced by the participants following
COVID-19 infection. Table 2 presents the frequency of symptoms and their
resolution. The most reported symptoms were ageusia (n=390), hyposmia/anosmia
(n=480), dizziness (n=230), headache (n=860), and loss of consciousness
(n=310).
Table 2: Frequency
and recovery rates of different COVID-19 neurological presentations.

Moreover,
a significant number of patients experienced severe neurological
manifestations, such as seizures (n=260), acute cerebrovascular events (n=500),
cerebellar syndromes (n=70), peripheral neuropathies (n=90),
meningitis/encephalitis (n=380), encephalopathies (n=380), neurological
syndromes such as Guillain-Barre syndrome (n=320), and spinal cord syndromes
(n=30).
A
statistically significant relationship was noted between ethnicity and
peripheral neuropathy (p=0·0001) as well as between ethnicity and neuro-syndromic
symptoms (p=0·001), with Asian patients being more likely to experience these
symptoms. Both sexes were statistically as likely to present with symptoms of
ageusia (p=0·0001), dizziness (p=0·033), gastrointestinal symptoms (p=0·0001),
and anorexia (p=0·0001). However, flu-like symptoms were statistically more
prevalent in females (p=0·008), whereas hyposmia (p=0·037) and haemoptysis
(p=0·0001) was more frequent in males.
Following
recovery from COVID-19 infection, a large proportion of patients demonstrated a
complete resolution of their symptoms. Specifically, patients presenting with
loss of consciousness and ageusia reported the highest resolution rates (93%
and 92% respectively), while the patients that experienced spinal cord
syndromes had the lowest resolution rates of their symptoms (33%).
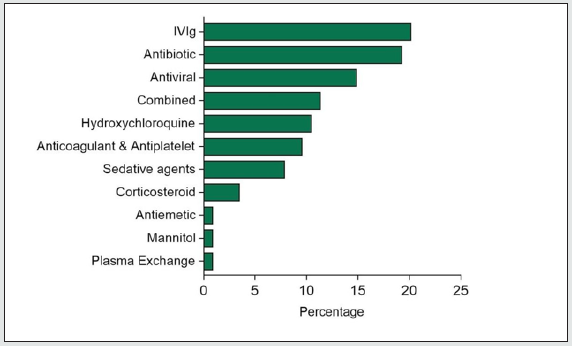
Treatments
The
most frequent treatments used in the studies analysed were intravenous
immunoglobulins (IVIG) (20·17%), followed by antibiotics such as azithromycin
(19·29%), antivirals (14·91%), and hydroxychloroquine (10·52%). However, a
combination of therapies was required for treatment in some patients. Figure 2
illustrates the different types of drugs that the COVID-19 patients received
during their admission and how the drug therapy is markedly heterogeneous among
this group of patients.
Figure 2: Drug type administered to COVID-19 patients.

The
most common route of drug administration was intravenous (65%), although oral
drug administration and intramuscular injections were also utilised. Patients
received treatment for a mean duration of 6 (±4) days.
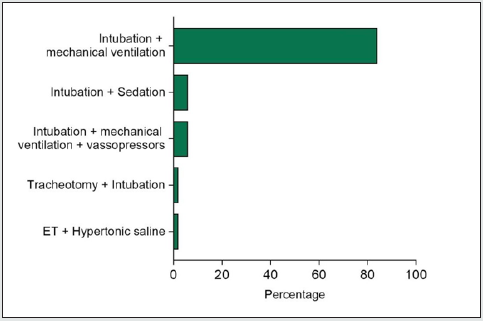
Prognosis
Patients
admitted to an Intensive Therapy Unit (ITU) were reported in 126 studies.
Figure 3 shows the different types of management that patients received when
admitted to ITU and illustrates that the most common cause of ITU admission was
the need for respiratory support with intubation and mechanical ventilation
(84% of the cases).
Figure 3: Types of ITU management received by patients.

ITU
admission was found to have a statistically significant relationship with males
(p=0·024), but not age. Interestingly, there was a statistically significant
relationship with ITU admission and symptoms of hyposmia/anosmia (p=0·0001),
headache (p=0·035), acute CVA (p=0·0001), seizure (p=0·001), meningitis
(p=0·034), and encephalopathies (p=0·0001).
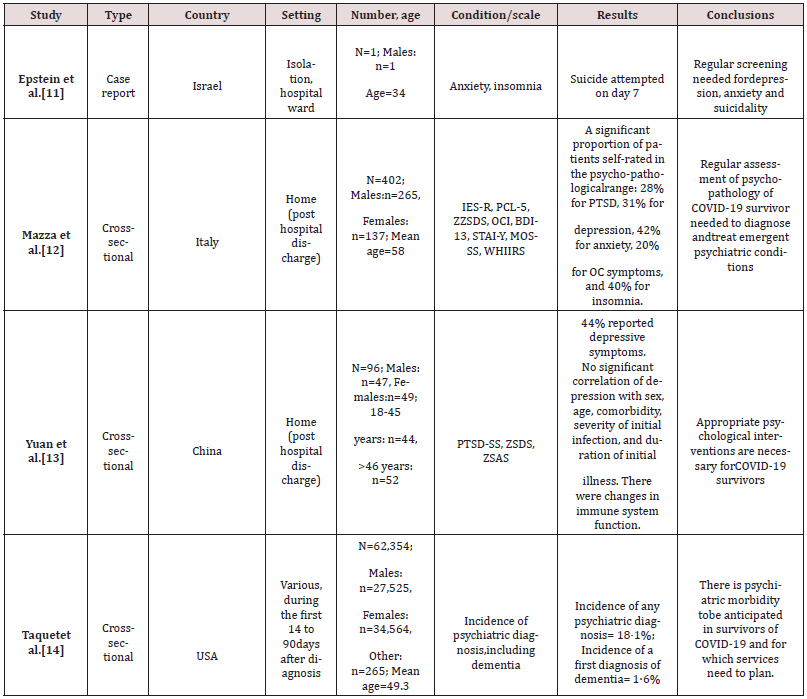
Psychiatric Symptoms
We
identified seven studies reporting psychiatric effects, of which five were
cross-sectional studies, one was a retrospective cohort study, and one was a
case report. Details of the six studies are reported in Table 3. The studies
involved 299,000 patients in total, of which 44% were male and 56% were female.
Half of the studies were reported in China. Three studies involved 171 patients
in hospital settings while having active COVID-19 infection, three studies
involved 498 patients at home after recovery, and one study involved 62,354
patients covering both inpatients during infection and those at home after
recovery. All studies identified depression and anxiety as being relevant to
COVID-19 infection, both during and after infection. Additionally, one study
reported suicidality during infection, two studies reported post-traumatic
stress disorder after infection, one study suggested obsessivecompulsive
disorder after infection, one study suggested insomnia after infection, one
study suggested a higher incidence of psychosis, and two studies suggested a
higher incidence of dementia diagnosis as being relevant to having been
diagnosed with COVID-19.
Table 3: Studies
reporting psychiatric effects related to COVID-19 infection.

Discussion
The
literature published on the neurological symptoms observed in patients with
COVID-19 is vast. Through our review, we aimed to summarise all available
literature, as well as include more recent studies that older reviews may not
have included. Our review specifically served to identify and examine the
frequency and severity of these symptoms through combining this existing
literature. In total, 307 neurological studies covering 60,097 patients, were
included in this systematic review, which has shown that COVID-19 is associated
with a large variety of neurological symptoms. The most frequently reported
symptoms included ageusia, hyposmia/anosmia, dizziness, headache, and loss of
consciousness. These symptoms are not specific to SARSCoV- 2 infection and are of
low severity, however they may suggest neurotropism. They also associate with
high resolution rates (all >80%). The most common severe neurological
complication of COVID-19 was acute cerebrovascular events. This result is in
keeping with other systematic reviews [18,19].
Direct
neurological damage including ischemic strokes, meningitis/encephalitis, or
Guillain-Barre syndrome are relatively common extra-pulmonary neurological
presentations according to our review. These results should be the springboard
for further research efforts aiming to distinguish whether these neurological
entities are a consequence of direct brain injury/infection or an interaction
with other vascular comorbidities of patients suffering severe/critical
COVID-19 disease.
A
significant proportion of COVID-19 patients were asymptomatic due to the course
of SARS-CoV-2 infection. In addition, patients may not present with respiratory
symptoms or fever but still have initial neurological manifestations. Thus,
when patients present with neurological symptoms, despite the absence of
respiratory symptoms, clinicians should maintain a high level of clinical
suspicion for the possibility of underlying COVID-19 asymptomatic infection.
The
resolution rates of neurological symptoms also varied. Patients presenting with
loss of consciousness and ageusia reported the highest resolution rates (93%
and 92% respectively), with ageusia resolution rates being 100% in one study
[20]. On the other hand, patients who experienced spinal cord syndromes, such as
acute myelitis, had the lowest resolution rates of their symptoms (33%). This
finding is supported by the established poor overall outcomes associated with
acute myelitis, with only approximately one-third of patients experiencing a
favourable outcome [21].
A
statistically significant relationship was noted between Asian ethnicity and
peripheral neuropathy. The relationship between ethnicity and peripheral
neuropathy in the context of COVID-19 has yet to be explored. However,
peripheral neuropathy as a complication of diabetes has been found to be more
prevalent among Caucasian patients [22] and less common in those with Indo-
Asian and African- Caribbean origins [23]. Moreover, a statistically
significant relationship was noted between Asian ethnicity and neuro-syndromic
symptoms. Nonetheless, it is important to note that both of these relationships
may have been influenced by the fact that the majority of the participants in
the studies included were Asian and that a number of papers did not disclose
the ethnicity of their participants.
Additionally,
flu-like symptoms were statistically more prevalent in females, possibly
because males have been found to have a higher risk of severe illness with
COVID-19 [24]. Hyposmia and haemoptysis were statistically more prevalent in
males. This is in contrast to several previous studies that found hyposmia to
be more common in females with COVID-19 infection [25-28]. However, our patient
cohort was predominantly male (62%), which may have contributed to the
differing results. Regarding haemoptysis, it is a very uncommon presentation
that was only present in 10 patients.
ITU
admission was found to have a statistically significant relationship with male
sex, but not with age. A meta-analysis of patients with COVID-19 also demonstrated
a relationship between sex and ITU admission, with male patients having almost
three times the probability of requiring ITU admission compared to females
[29]. Surprisingly, our study did not determine any relationship between age
and ITU admission. In contrast, another meta-analysis found that patients
greater than 70 years old have a higher risk of needing intensive care [30].
Furthermore, there was a statistically significant relationship between ITU
admission and the symptoms of hyposmia/anosmia, headache, acute CVA, seizure,
meningitis, and encephalopathies.
Treatment
varied, with several different therapies and drug routes being used depending
on the neurological manifestation and severity of the presentation. The most
frequent treatments used were intravenous immunoglobulins (IVIG), followed by
antibiotics such as azithromycin, antivirals, and hydroxychloroquine, with
patients receiving treatment for a mean duration of 6 days. A systematic review
assessing treatment strategies for COVID-19 similarly found antivirals,
antimalarials, and antibiotics to be the mainstay of treatment [31]. The
frequency of IVIG can be attributed to its use in treating many different
neurological conditions, most notably Guillain-Barre Syndrome, which was the fourth
most common neurological complication reported in this review. Finally, it is
important to consider that the COVID-19 pandemic is rapidly evolving and that
treatment options are continually being trialled and developed.
Even
though we established an abundance of studies for neurological symptoms, there
appears to be a lack of studies regarding the psychiatric effects during and
after COVID-19 infection. Nonetheless, all the studies we were able to identify
reporting psychiatric effects have found depression and anxiety to be relevant,
both during and after infection with COVID-19. In severe cases, there may even
be a risk of patients attempting suicide. Compared to people who had flu or
other respiratory tract infections, COVID-19 survivors were more likely to
receive a diagnosis of anxiety of depression over the same period [17]. It was
found that involving psychiatric care for these patients was effective in
reducing their symptoms of anxiety and depression. Without proper psychiatric
intervention, there is a risk that these psychiatric symptoms could increase
the risk of suicidal ideation. Overall, it is recommended that psychiatric
and/or psychological support should be available in hospitals to patients
admitted to medical wards due to COVID-19, as well as in the community
following recovery. This process may involve both the use of pharmacological
and/or psychological interventions. Given the fact that COVID-19 survivors were
at higher risk of receiving a diagnosis of dementia at 6-months follow-up, access
to memory clinics should also be available to this group of patients. More
studies examining the short-term and long-term psychiatric effects during and
after COVID-19 infection are required in the future to obtain a better
understanding of the symptoms, as well as to develop effective management
strategies.
Read More Lupine Publishers Neurology and Brain Disorders
Articles: https://brain-disorders-lupine-publishers.blogspot.com/